Cardiologia Croatica
Journal Research Assistant
Journal Research Assistant
Journal Research Assistant
Journal Research Assistant
Goran Krstačić, Mario Ivanuša, Vedrana Škerk
SUMMARY: As part of a public health initiative on the occasion of the 2014 World Heart Day, the Croatian Heart House and the City of Zagreb – the City Health Center at the Institute for Cardiovascular Prevention and Rehabilitation in Zagreb – organized preventive cardiovascular examinations for the persons between the ages of 40 and 60 that had not had a cardiac examination before. The goal of this initiative was to detect the traditional risk factors for cardiovascular diseases in the aforementioned group and to report the results of the conducted public initiative. Anthropometric measurements were conducted on all subjects (body weight, height, body mass index), fasting values of serum lipids and glucose were determined, 12-lead ECG was performed, and blood pressure pressure was measured. Following this, the participants were examined by either an internist or a cardiologist. The results were devastating: increased body mass index (BMI) was noted in 2/3 of the patients, as well as the presence of arterial hypertension (AH) in 45%, and hyperlipidemia in 55% patients. Men showed higher prevalence of unregulated AH, and women showed increased BMI. These results emphasize the problem and demonstrate the need for more frequent public health initiatives.
Mario Ivanuša
The second edition of the instructional booklet Heart failure by Gardner, McDonagh, and Walker brings 476 pages divided into seven parts with 42 chapters. The pocket format of this specialist-oriented edition is something Oxford University Press is well known for. The topic of the book is heart failure, one of the most common public health problems today. Heart failure is a growing problem around the world, and it is a cardiological disease whose increased incidence and prevalence are related to the aging of the population and improved treatment for coronary heart disease. The book opens with introductory information about this well-known syndrome, followed by chapters on chronic heart failure, comorbidities, acute heart failure, diagnostic and therapeutic procedures, implementation and a multidisciplinary approach, and palliative care for patients with acute decompensated heart failure. The book closes with an index of terms. The experienced team of Scottish educators divided the text to mirror the actual prevalence of specific forms of heart failure. Part one provides basic information on diagnosis, treatment, and the various types of chronic heart failure, taking up half of the book. The rest of the book resembles the fast onset of symptoms and signs that make up the clinical picture of heart failure, consisting of a quick succession of concise descriptions of clinical status, diagnosis, and treatment. The chapter on medical treatment focuses, as expected, on ACE inhibitors, beta-blockers, aldosterone antagonists, and diuretics. Clinical applicability of the contents and the modern illustrations are the most important reasons why you should choose this book. We recommend the book to cardiology specialists and residents in cardiology, internal medicine, and cardiac surgery, and it can also serve as a useful source of knowledge to nurses with a special interest or specialization in the heart failure.
Saida Rezaković, Mima Georgieva, Lidija Počanić
Abstract: Psoriasis is a chronic inflammatory disease affecting 1-2% of the adult general population. Disease is not limited only to the skin but is associated with a number of comorbidities, which significantly affect quality of life and present a higher risk of various medical disorders. Over recent years, numerous publications have shown increased frequency of cardiovascular disease and metabolic syndrome in patients with psoriasis. Although the etiopathogenetic relationship between these conditions is still not entirely clear, it seems that they share common pathophysiological elements in terms of similar inflammatory components. Considering the increased prevalence of cardiovascular comorbidities in patients, psoriasis should be approached as a multisystem disease. Therefore, a multidisciplinary approach is needed in order to most effectively manage patientswith psoriasis . In addition, cardiac drugs have been frequently reported to induce or exacerbate psoriasis, among which beta-blockers are found to be the most common triggering drug. It is thus important to acknowledge this relationship, as this is cutaneous drug adverse reaction which significantly affects quality of life and is a great psychological burden and stigma for the patient, as well as having a great impact on further treatment compliance.
Satoshi Nakatani
SUMMARY: The ‘Almanac’ Reviews provide an overview of articles on a specific topic published in Heart over the past 2 years, put in the context of advances in the field, including publications from several other journals. The focus of this Almanac article is Cardiovascular imaging — as a general cardiology journal, the imaging research in Heart tends to be clinically oriented and often will impact our clinical practice.
Oliver P Guttmann, Saidi A Mohiddin, Perry M Elliott
SUMMARY: Cardiomyopathies are myocardial disorders that are not explained by abnormal loading conditions and coronary artery disease. They are classified into a number of morphological and functional phenotypes that can be caused by genetic and non-genetic mechanisms. The dominant themes in papers published in 2012–2013 are similar to those reported in Almanac 2011, namely, the use (and interpretation) of genetic testing, development and application of novel non-invasive imaging techniques and use of serum biomarkers for diagnosis and prognosis. An important innovation since the last Almanac is the development of more sophisticated models for predicting adverse clinical events.
Jadranka Separovic Hanzevacki
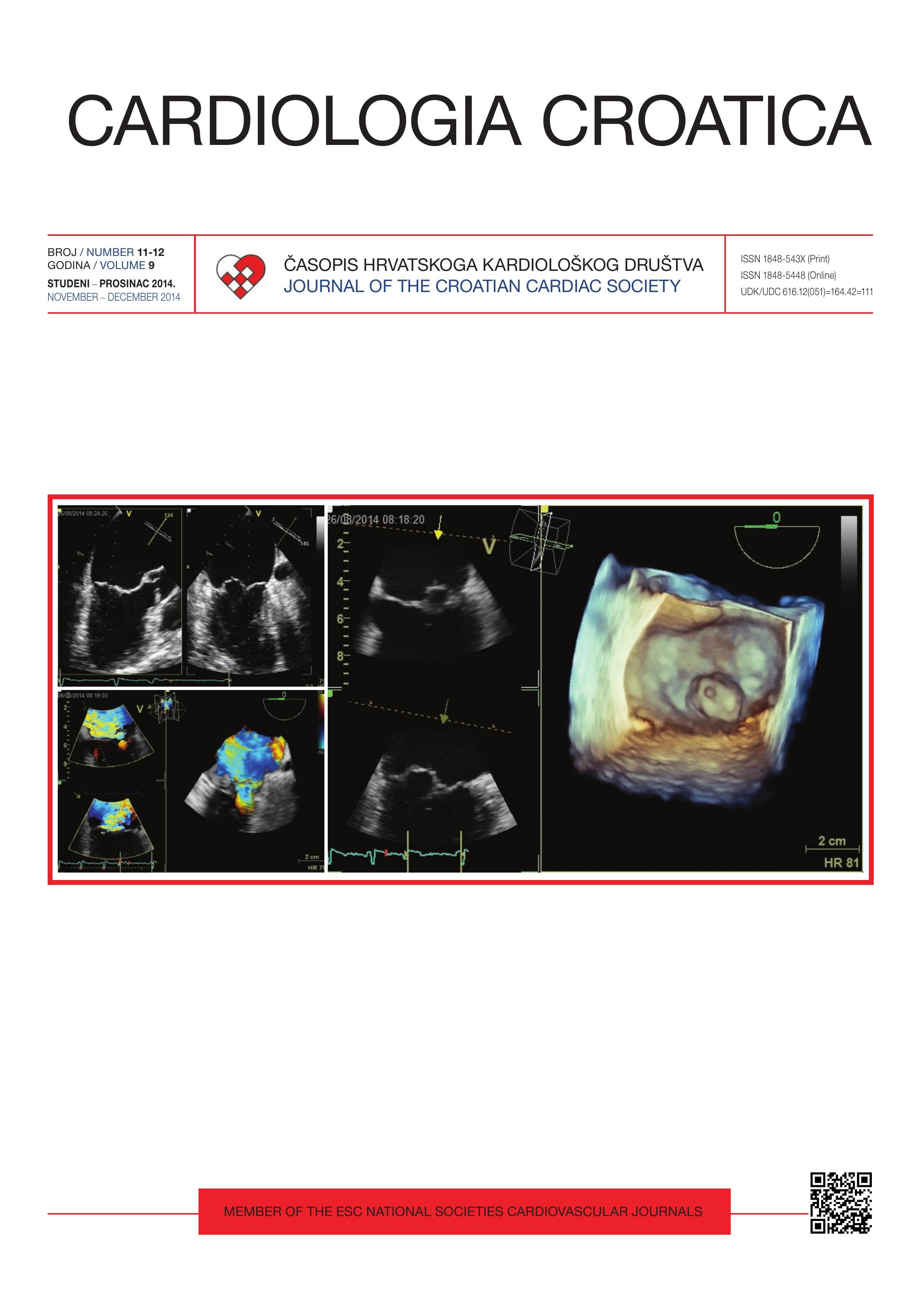
Due to many technological and scientific discoveries, echocardiography has developed into a complex diagnostic examination with a detailed protocol that uses numerous highly complex and demanding analyses and calculations (1). The development of echocardiographic methods and heart imaging in general has allowed better, faster, and more rational diagnosis and treatment of patients with cardiac problems. It is almost impossible to describe the complexities of this examination in the framework that dates back to 1992 and has never been expanded with a single procedure and method since then, despite the fact that the recommendations and guidelines of echocardiography have undergone several changes in the meantime and new modern methods have been developed (2, 3). To illustrate this, even the term used for this examination is outdated in the list of diagnostic and therapeutic procedures of the Croatian Institute of Public Health (4): “Echocardiography with Doppler echocardiography” is far behind the times, and should be changed to “Standard transthoracic echocardiography” which is the term used in professional circles both in Croatia and abroad. Along with basic hemodynamics, an ultrasound examination of the heart assessing the function and blood flow of the heart necessarily uses Doppler echocardiography (including continuous wave Doppler, pulsed Doppler, and color flow imaging) and is not complete without it (5). Assessing heart valve disease, myocardial function and hereditary diseases of the heart and surrounding structures, congenital heart diseases must include all the standard methods: one- and two-dimensional imaging (necessary for structure analysis and precise measurement) and Doppler echocardiography. **The examination is not complete if any of these standard methods is omitted.** Thus, echocardiography includes the use of Doppler echocardiography by definition, and cannot be called echocardiography without it. A basic orientational “heart viewing” is sometimes performed to establish a few urgent diagnoses, but it does not include Doppler echocardiography and thus surely cannot be considered identical to standard transthoracic echocardiography. As technology and medicine developed, in particular due to advancements in cardiology and echocardiography, heart ultrasounds have changed completely in terms of their components and terminology, and new methods and tests have been developed that are now used routinely (e.g. Doppler myocardial imaging, three-dimensional echocardiography, speckle tracking, etc.). Due to advancements in echocardiography both in Croatia and abroad, this valuable and irreplaceable cardiologic examination should be evaluated based on international expert recommendations. Several categories of echocardiography must be differentiated, depending on the time, expertise, staff, and technical requirements, evaluating existing expenses appropriately. In diagnosing complex patients, very complex diagnostic methods must be used. These include hemodynamic measurements and advanced echocardiographic procedures, which are: Doppler myocardial imaging, stress echocardiography, 2D stain imaging, optimization of the electrostimulator, and three-dimensional echocardiography (3). These are complex echocardiographic procedures that require more time, high expertise and technical requirements, and complex analysis (even more so than magnetic resonance imaging, for instance), and must thus be considered individually. This is why the American Society of Echocardiography categorizes echocardiographic examinations based on their complexity (orientational, simple, and complex). Considering all the above, it is extremely important to **standardize the basic echocardiographic examination**. In line with the recommendations of the European Association of Cardiovascular Imaging (1) and the development of cardiac diagnostics, the Working Group on Echocardiography and Cardiac Imaging Modalities of the Croatian Cardiac Society supports the standardization of echocardiographic examination as the first step to achieving consistent high quality echocardiographic results and their practicable application. This includes applying appropriate guidelines and evaluating medical personnel, with the interests of the patients and the overarching goal. Standardization of modern echocardiography should include the following:- **Continuous electrocardiographic monitoring**. An electrocardiogram enables timing of the various parts of the heart cycle, which is crucial for accurate measurement. Without the electrocardiogram, structure imaging and Doppler parameters will be incorrect, and lead to improper interpretation of the results.- **Respiration monitoring** during echocardiography using electrodes on the thorax. According to the recommendations from echocardiographic societies (1), electrocardiography is not complete without an assessment of the influence of respiration on basic hemodynamic events in the heart. It is crucial to determine the level of urgency in some lethal states.- Every measurement and piece of data obtained during echocardiography must be **archived and readily available**. Electrocardiographic examinations should be archived in digital format according to the recommended protocols of the European and American echocardiography associations, which define the contents and quality of the archived data as well as the technical and physiological conditions, including all image and quantitative data (1). (The recommended protocol of the Working Group on Echocardiography and the European Association of Echocardiography prescribes the contents of the examination as well as the conditions, methods, and contents of the results).- **The expertise of a specialist/subspecialist in the subsequent analysis** of the images. Determining the hemodynamics in the set intervals of the heart cycle sets echocardiography apart from other sonographic methods and makes it a very complex procedure in which the knowledge and expertise of a specialist are vital, just as in magnetic resonance imaging of the heart, computed tomography, etc. The job of the specialist includes performing the measurements, calculating the physical parameters of the basic hemodynamics, digital reconstruction of the structures in question, volume parameters in all phases of the heart cycle, archiving the data on portable data carriers for the patient’s use, and directly writing down the results at the workstation. The additional time spent after the examination is at least 30 minutes, and can range to several hours in complex cases. (Included are measurement preparations and calculating complex numeric variables for quantifying valve defects, pathological compounds, and indicators of the functional abilities of the ventricle according to the recommendations of the European Association of Echocardiography.)- The minimal timeframe for a standardized echocardiographic examination must be 30-40 minutes; patient appointment intervals must not be shorter than that. According to the Croatian Health Insurance Fund’s current guidelines (4), the health insurance price of diagnostic procedures for outpatients is lower than the lowest prices for the same procedures in Eastern European countries, and several times lower than other European countries, e.g. Great Britain, France, Sweden: (§100-150); Slovenia: (§70), Belgium (§70), Romania (§70). The price of echocardiography in Croatia is so low it **does not cover the costs** of all integral elements of modern echocardiography, and the work of physicians and echocardiography technicians is neglected. For instance, the costs of one-dimensional imaging or M-mode, excluded from the Croatian Institute of Public Health’s outline of the procedure in 2008, are not covered by the price. One-dimensional imaging is an integral part of the procedure and cannot be replaced with other types of imaging while adhering to expert rules and guidelines, so it is always used in echocardiographic examinations. Concerning two-dimensional imaging, the time and staff guidebook says that “Ö that method gives the same data as 1D echocardiography in two dimensions”. This emphasizes that the same structure is being shown in two dimensions, and does not imply that the data acquired using these two methods will be the same! This is because one-dimensional echocardiography has a temporal resolution (1000 Hz) which is not achievable using other methods, and is the only way to get accurate and adequately precise standard measurements as well as determine time intervals and morphological and dynamic analysis (6). In parallel with the advancement of echocardiography to completely new diagnostic levels and capabilities, the criteria of expertise for cardiologists performing the procedure have risen as well, due to the recommended accreditation of echocardiographic competence and skills at the national or European levels, which is a requirement for laboratory accreditation by the European Association of Echocardiography (7, 8). An additional challenge for the echocardiographic society is maintaining appropriate examination quality in the face of exponential growth of the (justified and unjustified) demand for echocardiographic examinations (9). **Medical priorities** must be considered in order to perform services in an acceptable timeframe with the goal of providing the best cardiologic care and avoiding serious health issues for the patients. In this way, the appropriate diagnostic procedures are performed in order to quickly and rationally establish a diagnosis despite the limited examination options and prohibitive costs. One of the possible ways to increase the maximum number of procedures that can be performed in the given circumstances is including other highly-educated professionals in the process of echocardiographic examination, in line with the examples of Great Britain and the USA; a high level of expertise in the management of technological and human resources incorporates a hierarchy system among the staff performing the procedure. Thus, the part of the procedure related to standardized protocol archiving can be performed by a highly educated echocardiographic technician while the cardiologist focuses on difficult measurements, reconstruction, diagnosis, and analysis. ## Acknowledgments Figures on cover by courtesy of Echocardiographic Laboratory University Hospital Centre Zagreb — Refferal Centre for Echocardiography, Croatian Ministry of Health; Mitral valve prolapse, Transesophageal echocardiography — multiplane, 3D and 3D Color Doppler reconstructions.
Jana Ljubas Maček
Heart failure, sometimes called acute decompensated heart failure, is a clinical syndrome that happens as a result of damage to the structure and function of the heart, which leads to a lack of oxygen in the tissue that manifests with typical symptoms (shortness of breath, swollen ankels, fatigue) and clinical signs (tachycardia, gallop rhythm, pulmonary congestion, increased venous pressure, etc.). Insufficient heart function results in weakened systolic and/or diastolic function of the left and/or right ventricle. There are many etiological factors behind heart failure (HF). Most common are myocardial diseases caused by coronary heart disease, accounting for 70% of all cases, followed by the consequences of hypertensive disease and a large group of cardiomyopathies, which can be hereditary (dilatative, hypertrophic, restrictive, spongiform, and arrhythmogenic right ventricular cardiomyopathy) or acquired (various forms of myocarditis, endocrine and infiltrative diseases). Heart valve diseases are also an important cause of HF. According to statistical data, 1-2% of the adult European population suffers from HF; the estimated prevalence in Europe is 3/1000, with a prevalence of >10% in persons older than 70. (1) According to these estimates, 43000 to 80000 people suffer from chronic HF in Croatia, and the incidence in people above the age of 65 grows to 10/1000 per year. In Europe as a whole, the number of patients with HF is about 10 million. Most HF is diagnosed in its chronic form, whereas episodes of acute HF are usually superimposed on the disease progression and are a common cause of hospitalization. Acute HF can be triggered by a deterioration of volume status balance or by disease progression. Today, the most common cause of acute HF is acute coronary syndrome, followed by arrhythmias, heart valve disease, and inflammatory heart diseases. According to the ALARM-HF study, hospital mortality due to acute HF was as high as 11% despite the application of modern diagnostic and treatment. (2) Cardiovascular diseases are the leading cause of morbidity and death in Croatia (in 2012 the mortality was 48.3%, and 48.1% in 2013), despite the fact that mortality has trended downward since 2003 and reached levels below 50% in 2009. (3) Circulatory system diseases are still the leading cause of death in Croatia (24.232 people died in 2013, and a ratio of 569.4/100 000, according to the Croatian Institute of Public Health). Cardiovascular disease is the dominant cause of morbidity and mortality in Croatia (the mortality percentage was 48.3% in 2012 and 48.1% in 2013), despite a significant trend of reduced mortality that started in 2003, with mortality reaching less than 50% in 2009. (3) Circulatory system diseases are still the primary cause of death in Croatia (24.232 people died in 2013, at a ratio of 569.4/100 000 inhabitants, according to data by the Croatian National Institute of Public Health). Tumors are the second most common cause of death (329.2/100 000). Cardiovascular disease is also a leading cause of hospitalization, with HF playing a significant role with a hospitalization rate of 117.5/100 000 (in 2013 5034 patients were hospitalized due to HF, 45.2% men and 54.8% women). Despite these high numbers, hospitalization due to HF is trending downward. The average duration of treatment for HF in Croatia is 11.4 days. (4) HF alone is a significant cause of morbidity and mortality and the 7th most common cause of death in Croatia: in 2013, 1341 people died of HF. Out of these, 63% were women, most likely because there are more women among the elderly. HF still has high rates of five-year mortality, with the likelihood increasing with the age of the patient. In patients above 65 as many as 94.8% died of HF, and 85% of those above 75 years of age. (4) Over the last 15 years, a HF-related mortality has trended down by about 60%, since 3306 deaths were registered in 1998, and only 1341 in 2013. This trend can be attributed to improved treatment of HF and other cardiovascular diseases, as well as earlier diagnosis. Since 2005, the Croatian Register of Heart Failure patients has collected data on patients with HF, which are available on-line from the Croatian Cardiac Society. (5) Before 1990, 60-70% of patients with HF died within 5 years of diagnosis, and repeated hospitalization due to worsening clinical symptoms was common, which placed a great burden on the health systems of many European countries. With the advent of modern therapeutic methods, a better rate of survival and a relative decrease in hospitalization of 30-50% was achieved, as well as a smaller but significant decrease in mortality. Many countries have noted an increase in the rate of hospitalization due to population being older in general, and an increase of prevalence is expected in countries where the age average is rapidly increasing. (1) HF treatment results vary depending on age group, gender, treatment options, and regional specificity. Pharmacological treatment and survival were better in patients treated by cardiologists and in younger patients as well as those that were men. (6) Treatment of chronic HF with standard medication is still the baseline treatment for most patients, and includes the use of ACE-inhibitors or angiotensin receptor blockers, beta-blockers, aldosterone antagonists, diuretics, and eventually digoxin and ivabradine. According to data from the Register of Heart Failure of the Croatian Cardiac Society, the most common medications used in treatment of HF are the following: diuretics (77%), beta-blockers (61%), ACE-inhibitors (48%), spironolactone (31%), digitalis (30%), and angiotensin receptor antagonists (21%). Beta-blockers significantly reduce the mortality and incidence of sudden cardiac death and improve the symptoms in patients with HF; however, beta-blockers are still not prescribed at an adequate level in many patients (with no developed side-effects). (7) Today, in addition to advances in standard medication therapies, a great deal of effort is being invested into discovering potential risk factors for sudden cardiac arrest in cardiomyopathies, especially in younger patients. Sudden cardiac arrest commonly happens in patients with mild existing symptoms, but can also happen before any clinical signs can be observed. In hypertrophic cardiomyopathy, the incidence of sudden cardiac death has decreased by 1% after 2010, but the prevalence of this condition is still very high at 1/500 (which would mean that 8874 persons are suffering from hypertrophic cardiomyopathy in Croatia). (8) Sudden cardiac arrest is associated with physical exertions in young athletes with hypertrophic cardiomyopathy, and appears in 0.06/100 000 cases per year (based on data from the last 27 years). In young athletes with some other form of heart disease it appears in 0.19/100 000 cases per year, and in as many as 0.71/100 000 cases in male athletes older than 15. (9) Cardioverter defibrillator implants have significantly reduced mortality from malign arrhythmias, but the mortality due to cardiomyopathy is still unacceptably high despite the introduction of advanced therapeutic methods such as cardiac resynchronization therapy (CRT), heart transplantation, and implanting ventricular assist devices (VAD). Despite a large number of available centers in Croatia (17 for pacemaker implants, 12 for AICD, 10 for CRT, and 3 centers undertaking electrophysiological studies and catheter ablations) and highly-educated personnel, the total number of implants is still low due to limited funds, adversely affecting the implementation of clinical practice guidelines in Croatia. In 2013, 2418 pacemakers, 81 CTS, and 156 AICD were implanted in Croatia. (10) Cardiac resynchronization therapy has been available worldwide since 2001 when the first cardiac resynchronization device was implanted. This extremely successful treatment for terminal HF is used in Croatia as well; 87 CRT devices were implanted in 2013, which makes for a modest 20 implants per million, far below the European Union average (140 CRT devices per million inhabitants). Since it became a member of the Eurotransplant organization (2008) and developed an desirable organizational model for organ transplants, Croatia has had one of the highest donor rates in Europe. In spite of that fact, there is still lack of donors and VADs have seen increased use and development. The first mechanical heart pump as a pre-transplant measure was implanted in 2008 at the University Hospital Centre Zagreb, and the program has grown since then. (11) Between September 2008 and October 2014, a total of 177 circulatory support system procedures were performed involving mechanical assistance to the heart, of which 165 in adults (a total of 135 patients) and 12 in children. Various pump models were used, including short-term extracorporeal veno-arterial membrane oxygenation (ECMO), short- to mid-term devices as a bridge to decision, transplantation, destination therapy or recovery, and in 2010 the first long-term VAD was implanted as a left ventricular assist device (LVAD). Since then, the HeartMate II pump has been implanted in 27 patients, and the most up-to-date HeartWare model in 5. On October 2, 2014, a total artificial heart was implanted for the first time in Croatia in UHC Zagreb; the patient is still in follow-up. In the US, such a procedure was performed for the first time in 2010. Today, two centers in Croatia perform heart transplants. The first heart transplantation in Croatia (and in Eastern Europe) was performed in 1988 in UHC Zagreb, where the treatment program for terminal HF has developed significantly, with 252 performed in the meantime. Most transplant patients suffered from ischemic cardiomyopathy (44.8%). The second most common indication was dilatative, idiopathic, or postmyocardial cardiomyopathy (31.7%). The third most common category of transplanted patients were performed on consisted of patients with other types of cardiomyopathies such as spongiform, hypertrophic, idiopathic restrictive cardiomyopathy, arrhythmogenic right ventricular dysplasia, and infiltrative diseases such as hemochromatosis and sarcoidosis. Only 5.6% of patients received a transplant due to secondary cardiomyopathy resulting from valve disease, and only 4.6% due to intractable coronary disease or as a consequence of acute myocardial infarction, according to the data from the Registry of Heart Transplant Patient in UHC Zagreb. Heart transplant programs have also been developing since 1995 in the Dubrava Clinical Hospital, with 121 performed to date. A number of new studies in the areas of pharmacological treatment, improvement in treatment possibilities of terminal HF, risk prevention for coronary heart disease, as well as education, better funding, and treatment availability form the basis for future advances in reducing morbidity and mortality from heart failure.
Janez Kopač, Mateja Grošelj, Breda Barbič-Žagar
SUMMARY: Krka has over 25 years of experience in the production of high-quality medicines acting on the renin-anigotensin-aldosterone system (RAAS) and has become one of the leading producers of them in Europe. Since its first introduction of a medicine acting on RAAS it has been performing international clinical studies in order to monitor the efficacy and safety of its products within the scope of the doctrine, enable doctors to gain their own experience with them, and prove their efficacy and safety in clinical practice. With the findings of the studies described in this article, we would like to present the contribution of Krka’s RAAS-acting medicines in the treatment of hypertension in over 25 years.